InformatiePrimaire endodontische behandeling Endodontische herbehandeling Bijzondere behandelingen Endo op een rijtjeWebwinkelBestel- en betalingsinformatie Eerdere aanbiedingen Handinstrumentarium Roterend instrumentarium Microscoop Accessoires Vulmaterialen Diversen Cursuspakket Beter Licht & ZichtOverigTrefwoorden Site map Presentaties (TIP!) Downloads Het Kanaal Links Endoplaza Forum MarketPlaza Over Endoplaza Gebruiksvoorwaarden site
|
The perforation
A surgery microscope
ad a: When a pulpa room is almost completely obliterated, it may be very difficult to find the remaining pulpa cavity. When striking fluid or blood the electronic length determinator When a perforation has been made, the location of the perforation can be checked with the aid of an X-ray. Over bone level the perforation can be closed with a plastic restoration, e.g. glasionomer cement. Under bone level the perforation is closed with MTA (Pro Root)   It is wise to look first further for the pulpa room and the canals before the perforation is closed. The survey should be optimal. When the pulpa room and the canal entrances have been found, gutta-percha styles 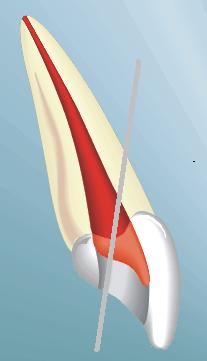 ad b: If a perforation is made while looking for the canals, the level of the perforation often lies lower than the pulparoom bottom or in the furcation (with molars). With incisives one mostly perforates towards buccal. Perforating towards lingual is out of the question. When looking for the canal, always prepare further to lingual. The electronic length determinator describes where exclusion/fixing or a perforation has been made. First, the real canals are searched and covered. Then, the perforation is closed with MTA (Pro Root). In the next session the endodontic treatment will be completed.
ad b: If a perforation is made while looking for the canals, the level of the perforation often lies lower than the pulparoom bottom or in the furcation (with molars). With incisives one mostly perforates towards buccal. Perforating towards lingual is out of the question. When looking for the canal, always prepare further to lingual. The electronic length determinator describes where exclusion/fixing or a perforation has been made. First, the real canals are searched and covered. Then, the perforation is closed with MTA (Pro Root). In the next session the endodontic treatment will be completed.ad c and d: Such (strip) perforations come into being if the endodontic opening is insufficiently wide over the canal entrances, or if one empties with too big instruments. Vijlen If in a bleeding canal a dry paper point ad e. An apical perforation arises when a ledge has been made, which entails a loss of length. The person in charge yet wants to come to length and continues filing with too thick, tough and not bent files, until all of a sudden it is easier to come to length. Then probably an apical perforation has been made. Measure with the electronic length finder determinator and then make a length picture. The place where the file comes out gives a reliable indication whether it is a perforation or that the usual canal has yet been made accessible. The perforation can be closed by placing a usual canal filling, or by placing MTA (Pro Root) if hand pluggers ad f. An older perforation has a worse prognosis. Often, a parodontal problem has already arisen which can be seen on an X-ray. Before such a perforation is closed, we cover it with CA(OH)2 at least a week to make the wound sterile. Then calcium sulfate (BoneGen)  Next the perforation is closed as described below in the outline. If there is a risk that MTA is pressed on while there is a big lucention near the perforation, first create a stopper with quickly hardening sterile calcium sulphate (plaster of Paris, BoneGen) and then place the MTA after you have cleaned the canal well again. Schematic enumeration closing perforations: |