InformationPrimary endodontic treatment Endodontic retreatment Special treatments Endodontics step by stepProduct catalogueOrder and payment information Previous special offers Hand instruments Rotary instruments Operating Microscope General instruments Accessoires Filling materials MiscellaneousRemainingReferences Site map Presentations (RECOMMENDABLE!) Downloads Het Kanaal Links Endoplaza Forum MarketPlaza About Endoplaza Instructions for use website
|
The open apex
There are various reasons why an open apex can be present and needs treatment, among others:
There are various methods to close off such an open apex: Until recently the open apex was almost closed off as a standard procedure by means of a so-called apexification with the help of Ca(OH)2. If then a dentine bridge had appeared, the canal filling was placed against it. This often was a long-lasting and time-consuming treatment, the favourable outcome was by far not always was certain. The latest method with the best prognosis is the closing off with MTA (Pro Root)  This happens as follows: In the first session, preparation and rinsing is done in the usual way. Then CA(OH)2 is placed in the root canal during at least a week. In the second session the root canal is again carefully cleaned. It is extremely difficult to remove CA(OH)2 from the canal. The surgery microscope 
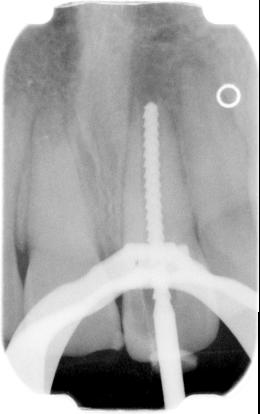

If it is a question of a big apical lucention which already was present for a long period, then there is much granulation tissue in the periapical area and there is no bone barrier. The barrier can be made by placing calcium sulphate (BoneGen) 



The last x-ray photo is 1 year after treatment.  In the third session the absorbent cotton is removed and the rest of the canal is filled as usual. From this page you can order in our web shop
to last chapter: Tracing perforations/fausse routes to next chapter: Filling the canals |